詳細
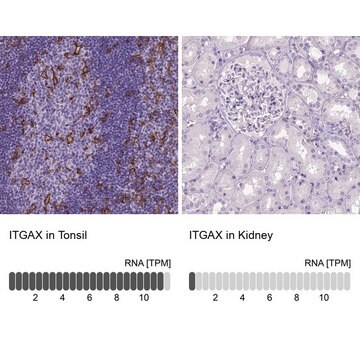
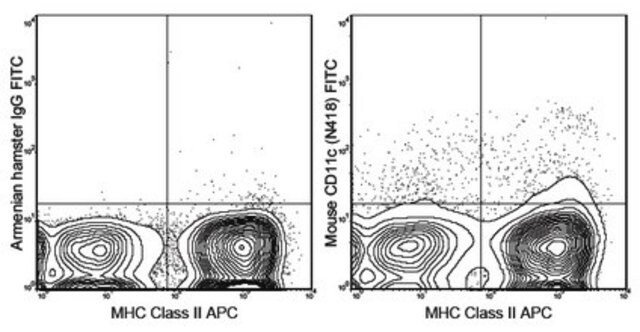
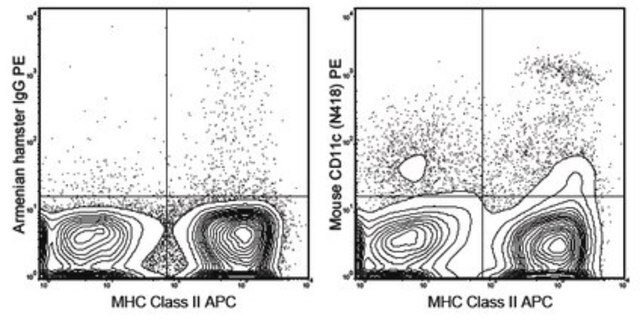
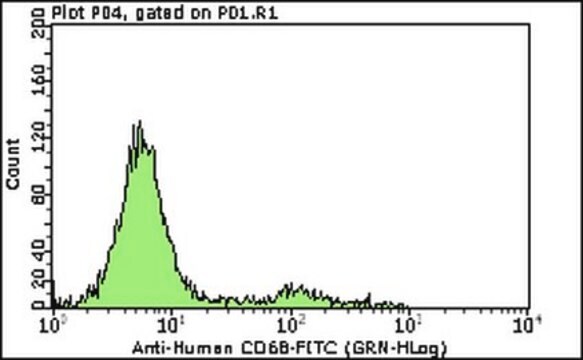
CD11c is an adhesion receptor of the leukocyte function-associated family of molecules. This cell surface antigen is normally expressed on granulocytes, monocytes, natural killer cells, and small populations of T- and B-lymphocytes. Therefore, the control for antibody validation and verification should be bone marrow and acute inflammatory tissue blocks. Anti-CD11c, clone 5D11, detects a formalin-resistant epitope of CD11c antigen and will now provide a significant change to the way hairy cell leukemia (HCL) can be diagnosed and assessed in FFPE. The tumor cells of the majority of other types of small B-cell lymphoma do not express this CD11c antigen. HCL is a distinctive yet uncommon chronic B-cell lymphoproliferative disorder, predominantly involving the bone marrow and spleen. Bone marrow aspiration and trephine biopsy are necessary for making a definitive diagnosis and treatment of hairy cell leukemia (HCL) although in exceptional cases, the diagnosis of HCL is made by histological analysis of splenic tissue after splenectomy or splenic needle core biopsy. However, aspiration is successful in only approximately 10% of patients. The marrow films obtained may demonstrate the presence of hairy cells but definitive diagnosis usually requires a bone marrow trephine biopsy due to the high frequency of a dry tap on aspiration. When there is difficulty in obtaining a good marrow aspirate, (frequent occurrence of a dry tap), examination of bone marrow trephine histology together with immunohistochemical analysis is the only available method to make a definitive diagnosis of HCL. Confirmation of the nature of the infiltrate can be obtained by immunocytochemistry performed on paraffin sections using antibodies against CD20, T bet, DBA.44 and TRAcP. However, expression of both TRAcP and DBA.44 (CD72) is not specific for HCL. It should also be noted, when undertaking immunohistochemistry to support a diagnosis of HCL in trephine biopsy sections, that up to 50% of cases show nuclear positivity for cyclin D1although confusion with mantle cell lymphoma (MCL) is less likely for an experienced hematopathologist as the cytology and histology of MCL are different from HCL. Korinna et al. in a recent study used clone (5D11) of anti-CD11c to investigate 31 bone marrow trephines with low-level HCL infiltrates and showed that the anti-CD11c was able to detect HCL to a level of 2% of tumor cells in BM biopsies. This indicates that immunohistochemical staining of formalin-fixed, decalcified bone marrow trephine biopsies with anti-CD11c can be used both for early diagnosis of HCL and for detection of residual disease following therapy. It is important to note that the CD11c-positive interstitial macrophages, which were generally more weakly stained than the hairy cells, did not interfere with the identification of the more strongly stained tumor cells. Among malignant lymphomas, CD11c is consistently expressed in HCL, although it is also rarely detected in B-CLL/small lymphocytic lymphoma, and nodal and extranodal marginal zone lymphoma (MZL).