
310M-2
Parathyroid Hormone (PTH) (MRQ-31) Mouse Monoclonal Antibody
About This Item
Polecane produkty



pochodzenie biologiczne
mouse
Poziom jakości
100
500
białko sprzężone
unconjugated
forma przeciwciała
culture supernatant
rodzaj przeciwciała
primary antibodies
klon
MRQ-31, monoclonal
opis
For In Vitro Diagnostic Use in Select Regions (See Chart)
Formularz
buffered aqueous solution
reaktywność gatunkowa
human
opakowanie
vial of 0.1 mL concentrate (310M-24)
vial of 0.5 mL concentrate (310M-25)
bottle of 1.0 mL predilute (310M-27)
vial of 1.0 mL concentrate (310M-26)
bottle of 7.0 mL predilute (310M-28)
producent / nazwa handlowa
Cell Marque®
metody
immunohistochemistry (formalin-fixed, paraffin-embedded sections): 1:100-1:500
izotyp
IgG2a
kontrola
parathyroid tissue
Warunki transportu
wet ice
temp. przechowywania
2-8°C
wizualizacja
cytoplasmic
informacje o genach
human ... PTH(5741)
Opis ogólny
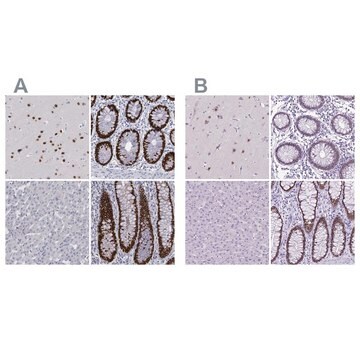
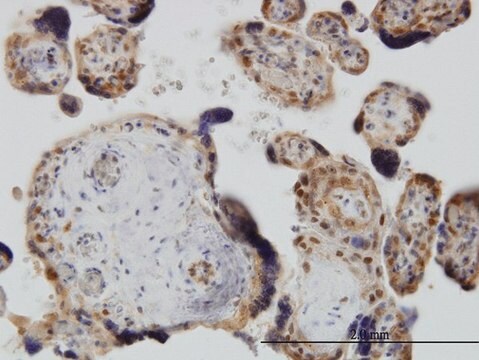
Surgical pathologists are familiar with the ability of parathyroid proliferations to assume a variety of histological guises, posing difficulty to categorize any given lesion as hyperplastic, adenomatous or carcinomatous in nature (Wick et al, 1997). This is usually resolved with macroscopic appearance of the remaining parathyroid glands as assessed by the surgeon. The role of the surgical pathologist is to identify the lesion as parathyroid in nature and to assess whether it is normocellular or hypercellular. Although easily accomplished in the majority of instances, rare examples of parathyroid hyperplasia/adenoma showing a follicular/trabecular arrangement may cause concern over the alternative diagnosis of a thyroid adenoma. This becomes more pertinent when the parathyroid lesion abuts into the thyroid gland or lies within the thyroid capsule. Immunostaining for thyroglobulin and parathyroid hormone (PTH) is especially useful to resolve the problem (Permanetter et al, 1983). Nevertheless, caution should be exercised since parathyroid cells often discharge their hormonal product almost as soon as it is packaged in the cytoplasm, resulting in false-negative anti-PTH immunostaining, although the cells are biologically synthetic (Wick et al, 1997)
Anti-PTH antibody is also useful to distinguish parathyroid hyperplasia/neoplasms from thyroid and metastatic neoplasms (Wick et al, 1997); although the pathologist is typically aware of the preoperative hypercalcemic status. Occasionally when the surgeon does not supply this information PTH immunohistochemistry is essential. Even more problematic, are situations in which clear cell parathyroid carcinomas are nonsecretory without an abnormality in mineral metabolism (Aldinger et al, 1982). In such situations, metastatic renal cell carcinoma or metastatic clear cell carcinoma of the lung is evident warranting PTH immunohistochemistry to arrive at the correct diagnosis (Wick et al, 1997). The other instance in which anti-PTH antibodies are useful is in the consideration of parathyroid carcinomas located primarily in the anterior mediastinum (intrathymically). In this situation distinction from primary thymic metastatic carcinomas, non-Hodgkin′s lymphoma and germ cell tumors is necessary (Murphy et al, 1986).
The diagnosis of the majority of parathyroid proliferation may be accomplished with an adequate history, biochemistry profile, and histomorphological assessment; however, rare instances in which the tumors have an abnormal location, clear cell morphology, or a non-secretory may result in erroneous diagnoses, warranting anti-PTH immunohistochemistry.
Jakość
 IVD |  IVD |  IVD |  RUO |
Powiązanie
Postać fizyczna
Uwaga dotycząca przygotowania
Inne uwagi
Informacje prawne
Nie możesz znaleźć właściwego produktu?
Wypróbuj nasz Narzędzie selektora produktów.
Kod klasy składowania
12 - Non Combustible Liquids
Klasa zagrożenia wodnego (WGK)
WGK 2
Temperatura zapłonu (°F)
Not applicable
Temperatura zapłonu (°C)
Not applicable
Wybierz jedną z najnowszych wersji:
Certyfikaty analizy (CoA)
Nie widzisz odpowiedniej wersji?
Jeśli potrzebujesz konkretnej wersji, możesz wyszukać konkretny certyfikat według numeru partii lub serii.
Masz już ten produkt?
Dokumenty związane z niedawno zakupionymi produktami zostały zamieszczone w Bibliotece dokumentów.
Nasz zespół naukowców ma doświadczenie we wszystkich obszarach badań, w tym w naukach przyrodniczych, materiałoznawstwie, syntezie chemicznej, chromatografii, analityce i wielu innych dziedzinach.
Skontaktuj się z zespołem ds. pomocy technicznej